INR Finger Stick Machines
INR Finger Stick Machines
If you participate on our Facebook page then you probably already know the stand that the APSFA takes regarding finger stick machines for testing APS patients’ INRs—finger stick machines are not accurate for APS patients.
Unfortunately, over half of the APSFA board of directors have had experience with erroneous INR readings from a finger stick machine. Luckily, the errors did not result in life altering, but when the numbers are off it can be the difference between holding a dose of a blood thinner or having a clotting event such as a stroke.
This is not a risk we are willing to take and not a risk we want other APS patients to take without being educated. This information has been on our links page for some time, but we decided it was time to take a formal stance.
We have been approached by vendors offering us advertising bids for thousands of dollars. We have turn them down. It is against our ethical standards to promote something that could harm or even kill you. You are worth more to us than that money. There are more ethical ways to raise money for our mission. Your safety will always come first in our eyes.
On this page is a compilation of articles, brochures, and links from many different sources on APS patients and INR (finger stick) machines. If nothing else, please educate yourself and call the manufacture to ask them point blank if they are accurate for APS patients. Thank you.
INR Machine Facts for APS Patients
Devices for ambulatory and home monitoring of blood pressure, lipids, coagulation, and weight management, part 2
Am J Health Syst Pharm.2005; 62: 1894-1903. Kelly L. Scolaro, Pamela L. Stamm and Kimberly Braxton Lloyd Copyright © 2005 by the American Society of Health-System Pharmacists.
INR Self Testing
INRs from POC instruments are unreliable in about 1/3rd of patients with the clotting disorder called antiphospholipid syndrome (APLA syndrome) who are on warfarin. In these patients, the POC devices give INR readings that are too high, or the instruments report error messages. This is the case with any of the 3 instruments on the market. If you have APLA syndrome, your INRs should be checked from blood drawn from a vein and tested in a laboratory.
Patient Variables in PT/INR Testing with INRatio
Technical Bulletin from HemoSense makers of INRatio. Clearly states that APS effects its results. The APSFA does not promote, sell or make money from this company nor the vendors that sell them. However, if this document has been relocated again, please feel free to contact us for it.
My Experience with Finger Stick (Home) INR Machines
Patient’s story on her use of a Home INR Machine and supporting company information.
MAUDE Adverse Event Report
Discrepant results (accuracy) comparison of inratio test with lab results provided by end-user at time complaint was filed: date: early 2007, inratio: 2. 1, lab: 8. 5, mean: 5. 3, confidence limits: unable to be determined. Per internal procedure, the mean of the inratio meter and comparative system inr were calculated. The confidence limits cannot be determined. The readings are considered inaccurate based on “area outside the acceptance region” table. The results are considered discrepant within the context of the documented variability for inr testing. Therefore, further testing is required at this time. In troubleshooting found that the pt has antiphospholipid syndrome. It was explained that possible interferences may be due to the varying levels of the antibodies. Pts condition may cause the discrepant errors.
Antiphospholipid Syndrome (APS) – NO to Home INR Machines!!
I started this blog to help get the word out that Home INR machines are NOT safe to use for patients with Antiphospholipid Syndrome. If you have APS, please read! Thanks!
INRatio Monitor and Interfering Substances
Anti-phospholipid antibodies can disrupt the phospholipid in the PT reagent that is necessary for the clotting reaction to occur thus artificially elevating the INR. The APSFA does not promote, sell or make money from this company nor the vendors that sell them. However, if this document has been relocated again, please feel free to contact us for it.
Thoratec Receives FDA Warning Letter, Plans Recall (ProTime)
Thoratec’s International Technidyne Corp. (ITC) division has received an FDA warning letter citing concerns about its quality systems, specifically those related to certain lots of its ProTime System anticoagulation monitoring device…..of incorrect readings of patient blood coagulation levels.
CoaguChek XS System – Patient Experience
Registration Required to read story. “I called Roche and expressed my concerns about the reliability of the machine. They told me that at higher INRs (above 4.0) the machine becomes less reliable. They also told me that the machine doesn’t work very well for people with Antiphospholipid Antibodies because these same antibodies are on the test strips! She said that especially when someone with APS is having a flare up the machine may not work well due to the high level of antibodies in the blood.”
i-STAT® PT/INR test
The i-STAT® PT/INR test is a whole blood determination of the prothrombin time used for monitoring oral anticoagulant (warfarin) therapy. The test determines the time required for complete activation of the extrinsic pathway of the coagulation cascade when initiated (activated) with a thromboplastin. Those using this machine should be getting vein draw comparisons at least every 6-8 weeks.
ProTime Systems
Representatives clearly state that this machine has problems with APS patients and patients with the Lupus Anticoagulant. Waiver for patients with APS must be signed. Those using this machine should be getting vein draw comparisons at least every 6-8 weeks. The APSFA does not promote, sell or make money from this company nor the vendors that sell them.
MAUDE Adverse Event Report
Discrepant results (accuracy) comparison of inratio test with lab results provided by end-user at time complaint was filed: date: 01/05/07, inratio: 6. 1, lab: 3. 8, mean: 4. 95, confidence limits: 2. 8-7. 2. Date: 01/15/07, inratio: 4. 3, lab: 2. 8, mean: 3. 55, confidence limits: 2. 2-5. 3. Per internal procedure, the mean of the inratio meter and comparative system inr were calculated. Both inratio and lab values are within the confidence limits for inr testing. The results are not considered discrepant within the context of the documented variability for inr testing. Therefore, further testing is not required at this time. Per text “pt has antiphospholipid antibody syndrome, (cardiolipin-positive, lupus-negative). ” pt’s condition may be causing interference.
INRatio by Alere formerly Hemosense
Representatives & Literature clearly states that this machine has problems with APS patient and patients with the Lupus Anticoagulant. Please see: https://apsfa.org/docs/HemoSense%20TechBull108.pdf Those using this machine should be getting vein draw comparisons at least every 6-8 weeks. The APSFA does not promote, sell or make money from this company nor the vendors that sell them. However, if this document has been relocated again, please feel free to contact us for it.
Validity of Criteria Used to Evaluate Fingerstick Devices That Assess International Normalized Ratio
Medical Decision Making, Vol. 26, No. 3, 239-246 (2006). Conclusion. The unvalidated criteria used to predict warfarin dosing agreement between 2 INR measurements are associated with large error. Warfarin dosing decisions should be measured directly in such assessments.
MAUDE Adverse Event Report
Caller alleged discrepant results compared with the lab. Results as follows: date: 01/12/07, inratio: 6. 1, lab: 3. 6. Ts updated this case on 01/18/2007 and 01/19/2007. 01/17/07, first test inr = 7. 5(old strip). Second test inr = 5. 5(new strip). Date: 01/19/07, inratio: 6. 5, lab: 4. 0. Caller has antiphospholipid syndrome and recently had an episode of multi organ infection resulting in failure of adrenal glands.
*INR Monitoring in Patients with Antiphospholipid Antibodies with Finger Stick INR Machines.
by: Stephan Moll, MD. A superb way to monitor INRs (International Normalized Ratio) in patients on oral anticoagulants who do NOT have antiphospholipid antibodies (APLA) is though use of “point of care instruments”, where the INR is tested on blood from a finger stick. This method gives fast results and is used by many physicians’ offices and by some patients at home. However, in patients with APLA on oral anticoagulants these instruments may give inaccurate readings.
CoaguChek & CoaguChek S Strip Insert
Literature clearly states that this machine has problems with APS patient and patients with the Lupus Anticoagulant. This is for the CoaguChek & CoaguChekS. Please call technical support at 800-428-4674 for more information. Those using this machine should be getting vein draw comparisons at least every 6-8 weeks. The APSFA does not promote, sell or make money from this company nor the vendors that sell them.
CoaguChekXS Strip Insert
Literature clearly states that this machine has problems with APS patient and patients with the Lupus Anticoagulant. This is for the new CoaguChekXS. Please call technical support at 800-428-4674 for more information. Those using this machine should be getting vein draw comparisons at least every 6-8 weeks. The APSFA does not promote, sell or make money from this company nor the vendors that sell them.
Factors That Influence INR system Comparisons
List includes Antiphospholipid Antibodies. The APSFA does not promote, sell or make money from this company nor the vendors that sell them. However, if this document has been relocated again, please feel free to contact us for it.
Hemochron Jr. Package Insert
Literature clearly states that this machine has problems with APS patient and patients with the Lupus Anticoagulant. Those using this machine should be getting vein draw comparisons at least every 6-8 weeks. The APSFA does not promote, sell or make money from this company nor the vendors that sell them.
Point-of-care testing of the international normalized ratio in patients with antiphospholipid antibodies.
SL Perry, GP Samsa, and TL Ortel Thromb Haemost, December 1, 2005; 94(6): 1196-202. Antiphospholipid antibodies can influence the results of clotting tests in a subset of patients, which can be a major obstacle in monitoring warfarin.The aim was to determine if point-of-care testing of the International Normalized Ratio (INR) is influenced by antiphospholipid antibodies. Please note the manufacture of this machine helped fund this study.
ProTime Microcoagulation System Package Insert
Literature clearly states that this machine has problems with APS patient and patients with the Lupus Anticoagulant. Those using this machine should be getting vein draw comparisons at least every 6-8 weeks. The APSFA does not promote, sell or make money from this company nor the vendors that sell them.
Coagucheck accuracy?
A long discussion about non-APS patients have accuracy issues with their finger stick readings, some of which had complications due to those inaccurate readings.
Alere INRatio® PT/INR Test Strips Package Insert
Lupus or antiphospholipid syndrome (APS) may falsely prolong the INR value. Testing with an APS-insensitive laboratory method is recommended for these patients.
Patient Education Blog | Clot Connect has posted a new item, ‘INR Self-Testing’
INRs from POC instruments are unreliable patients with the clotting disorder called antiphospholipid syndrome (APLA syndrome) who are on warfarin [ref 7]. In these patients, the POC devices give INR readings that are too high, or the instruments report error messages. This is the case with any of the 3 instruments on the market. If you have APLA syndrome, your INRs should be checked from blood drawn from a vein and tested in a laboratory. That value can then be compared to the INR obtained with a POC instrument from a finger stick. Only if both values correlate well may it be acceptable for you to use the POC machine for self-testing.
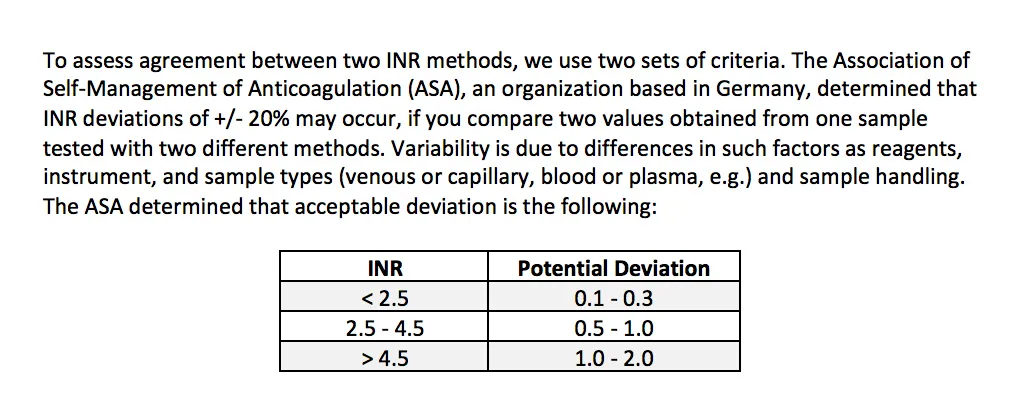
Anti-phospholipid Syndrome and PT/INR
Based on the conclusions of the studies mentioned, different methods of measuring PT/INR behave differently with different APA patients. It is therefore very important to assess the individual patient together with the responsiveness of the PT/INR reagent/system to be used to monitor warfarin therapy (lab or POC). It is also important when performing a correlation study comparing one PT/INR system to another to consider whether any of the patients included in the study have Anti-phospholipid Syndrome. The presence of such samples in the population may affect the correlation.
59 patients impacted by blood test error at Indian Head Union Hospital
The error was discovered because of changes to the reagents ” a substance that is mixed with a patient’s blood to do the test. When the region couldn’t get reagent for some aging equipment, senior technologists started to call around to find out how much reagent the rural sites had on hand and the testing error was discovered. About five rural labs need machines replaced. “We’re going to be rethinking our equipment needs in the rural sites as a whole,” Ledingham said. “Whether each of those five individual machines are going to be replaced or perhaps some of them will be serviced from a central site ” it will really depends on the needs of the patients and the clinicians in those communities.”
Accuracy Concerns on Testing Device for Blood-Thinning Drug
Dr. Gary Goldstein, a Florida internist, knew something was wrong with a blood-testing device in his office when, all of a sudden, it began giving out odd results.
An Advanced MAUDE Search
It is just not APS Patients anymore with inaccurate readings.
FDA Examines Safety of INR Point-of-Care Tests
By Amy Orciari Herman; Edited by Susan Sadoughi, MD, and André Sofair, MD, MPH.
The FDA convened a panel of experts on Friday to examine the accuracy of point-of-care tests to measure international normalized ratio (INR) in patients taking warfarin, the Wall Street Journal reports.
The agency says such tests have performed poorly in thousands of patients since their approval, with potentially false readings linked to 18 deaths in 2014 and 2015.
Two such tests, INRatio and INRatio2, were withdrawn from the market in 2014 over concerns that they gave faulty readings. INRatio has recently received much attention over its use in the ROCKET AF trial, which led to approval of the anticoagulant rivaroxaban (Xarelto). Critics assert that in ROCKET AF, falsely low INR readings with INRatio would have prompted higher warfarin doses—resulting in higher bleeding risks with the drug and thus making rivaroxaban seem relatively safer. The researchers reanalyzed their data, however, and concluded that the test did not significantly affect the trial’s primary outcomes.
Inaccurate Results from INR Meters Prompt New Information from FDA
The U.S. Food and Drug Administration (FDA) has published new information on the agency’s website for people who take warfarin (a blood thinner) and use portable, battery-operated INR test meters to monitor their therapy. This update was prompted by reports that some INR test meters may have generated inaccurate results. The FDA regulates INR test meters and test strips, and the agency wants to make sure all people who use these home-testing devices, regardless of make or model, are using them safely.
INR Management of an Antiphospholipid Syndrome Patient With Point-of-Care INR Testing
Management of patients with antiphospholipid syndrome on warfarin therapy can be challenging. The international normalized ratio (INR) of patients with antiphospholipid syndrome can be falsely elevated. This elevation is thought to be reflective of the reaction of the antiphospholipid antibody with the thromboplastin used to measure the protime. This false elevation can be seen in both venipuncture and point-of-care results. This discrepancy is usually more apparent in patients with whose INR is tested using point of care. As a result, there is a preference for venipuncture INR testing in most patients with antiphospholipid syndrome requiring warfarin therapy. In our case, we highlight one patient who we correlated her venipuncture INR with point-of-care INR as well as a chromogenic factor X level in order to manage her INR by point-of-care INR testing.
Coagsense correlated better than Coagucheck XS and did not show increasing bias as INR increased. Both POC instruments had higher INR variability in 4 disease states (antiphospholipid syndrome, autoimmune, peripheral vascular disease, and hypercoagulable). Patient-specific laboratory correlations may be needed on each POC device.
Accuracy of CoaguChek XS in Patients With Antiphospholipid Syndrome
The CoaguChek XS meter is an international normalized ratio (INR) point-of-care (POC) monitor that has been shown to provide clinically acceptable accuracy. Because of a potential interaction between antiphospholipid antibodies and the reagent used in the prothrombin time INR assay, there is uncertainty as to the reliability of using POC INR monitors in patients with antiphospholipid syndrome (APLS). The study population consisted of 41 patients on warfarin therapy for either APLS (treatment group) or any other indication (control group). All patients had their INR analyzed by the CoaguChek XS meter and a central laboratory. Overall, the mean INR difference between the CoaguChek XS and laboratory in the APLS patients was 0.6772 (P < 0.0001). In APLS patients, when the laboratory INR was less than 2.0, 2.0 to 3.0, 3.1 to 4.0, or greater than 4.0, the CoaguChek XS differed by averages of 0.0636 (P = 0.4111), 0.6903 (P < 0.0001), 1.1417 (P < 0.0001), and 0.9333 (P = 0.0848), respectively. In the control group the overall mean difference was 0.5456 (P < 0.0001). For laboratory INR values of less than 2.0, 2.0 to 3.0, 3.1 to 4.0, and greater than 4.0, the mean differences from the CoaguChek XS were 0.3000 (P = 0.0003), 0.4444 (P < 0.0001), 1.0444 (P = 0.0002), and 1.3500 (P = 0.0236). Our data do support the manufacturer recommendation of comparing laboratory and CoaguChek XS meter INRs in APLS patients because in a subset of patients the 2 methods produced acceptable results, and POC monitoring might be used.
Antiphospholipid Syndrome: Diagnosis and Management
Antiphospholipid antibodies can lead to falsely elevated INR results (most common with point-of-care devices). Confirming the factor X activity (using a chromogenic assay) can be useful to calibrate the target INR range.
Conclusion: There is a disagreement between INR values measured with the CoaguChek XS and laboratory-INR in a proportion of patients with LA. Consequently, laboratory-INR monitoring should be preferred over POCT-INR monitoring in patients with LA-positive APS, especially in patients with high anti-β2-glycoprotein IgG antibody titers. Published Date: 1/2023
Coag Sense Professional Manual
What can cause unexpected results?
Certain prescription drugs (for example, heparin) and certain over-the-counter medications (for example, antibiotics) can affect the action of oral blood thinners and the INR value.
Changes in diet, lifestyle, or taking nutritional supplements such as ginkgo biloba can affect the action of oral blood thinners and the INR value. Liver diseases, congestive heart failure, thyroid dysfunction, Lupus, antiphospholipid antibody syndrome (APS), and other diseases or conditions can affect the action of oral blood thinners and the INR value.
Be sure to confirm whether the patient has any of these conditions before you begin testing, and any time there are changes in patient health status or medications after you have begun testing.
What to do when you get an unexpected result:
Follow instructions for re-testing on the Coag-Sense PT/INR meter. For unexpected results, contact Technical Support at 1-866-903-0890. Consider re-testing using an alternative method prior to adjusting the patient’s dose of anticoagulant medication or any other corrective actions.
Conclusions: In a subset of patients with APS who, during self-managed VKA therapy, had persistently higher
POCT INR than P-INR, the majority could continue with self-managed therapy using a conversion table, as the
falsely elevated POCT INR values were linearly correlated to P-INR. Published Date: Thrombosis Research, Volume 252, 109361, August 2025
There was an allegation of questionable results from the Coaguchek Xs meter, serial number (b)(6).At 11:15 am, the meter result was 1.7 inr. At 11:41 am, the meter result was 2.4 inr. The customer’s therapeutic range is 2.0-3.0 inr. Customer tests on a weekly basis.
Conclusion: Coagsense correlated better than Coagucheck XS and did not show increasing bias as INR increased. Both POC instruments had higher INR variability in 4 disease states (antiphospholipid syndrome, autoimmune, peripheral vascular disease, and hypercoagulable). Patient-specific laboratory correlations may be needed on each POC device. Citation: Point of Care: The Journal of Near-Patient Testing & Technology 19(1):p 12-18, March 2020. | DOI: 10.1097/POC.0000000000000197
Conclusion: There is a disagreement between INR values measured with the CoaguChek XS and laboratory-INR in a proportion of patients with LA. Consequently, laboratory-INR monitoring should be preferred over POCT-INR monitoring in patients with LA-positive APS, especially in patients with high anti-β2-glycoprotein IgG antibody titers. Citation: Res Pract Thromb Haemost. 2023;7:e100011 www.rpthjournal.org – 1 of 8 https://doi.org/10.1016/j.rpth.2022.100011
Tips for using INR test meters at home for patients and caregivers
When a patient expresses a desire for in-home testing, the reason for their anticoagulation must be considered. Some blood illnesses, such as antiphospholipid syndrome (APLS), interfere with how the system evaluates INR ratings. Therefore, point-of-care testing is preferred not to be conducted on those individuals. Date: December 1, 2021
INR results from patients treated with Direct Oral Anticoagulants (DOACs) e.g rivaroxaban, apixaban, edoxaban, betrixaban and dabigatran may be influenced and should be confirmed with an alternative laboratory method
Note: Samples from patients treated with the following drugs must not be tested with the system: protamine sulfate, oritavancin, calcium dobesilate
The action of oral anticoagulants (coumarin derivatives) can be increased or weakened when other medication is taken simultaneously (e.g. antibiotics but also prescription-free medication like pain relievers, antirheumatic medication and medication against influenza). This, in turn, can also lead to either an increase or a decrease in prothrombin time (INR). If other medication is taken, it is recommended that the prothrombin time be checked more frequently and that the anticoagulant dose be subsequently adjusted
The presence of anti‑phospholipid antibodies (APAs) such as Lupus antibodies (LA) may lead to prolonged clotting times, i.e., they may cause false‑high INR values. If you have or suspect that you have APAs, discontinue testing until you discuss with your physician
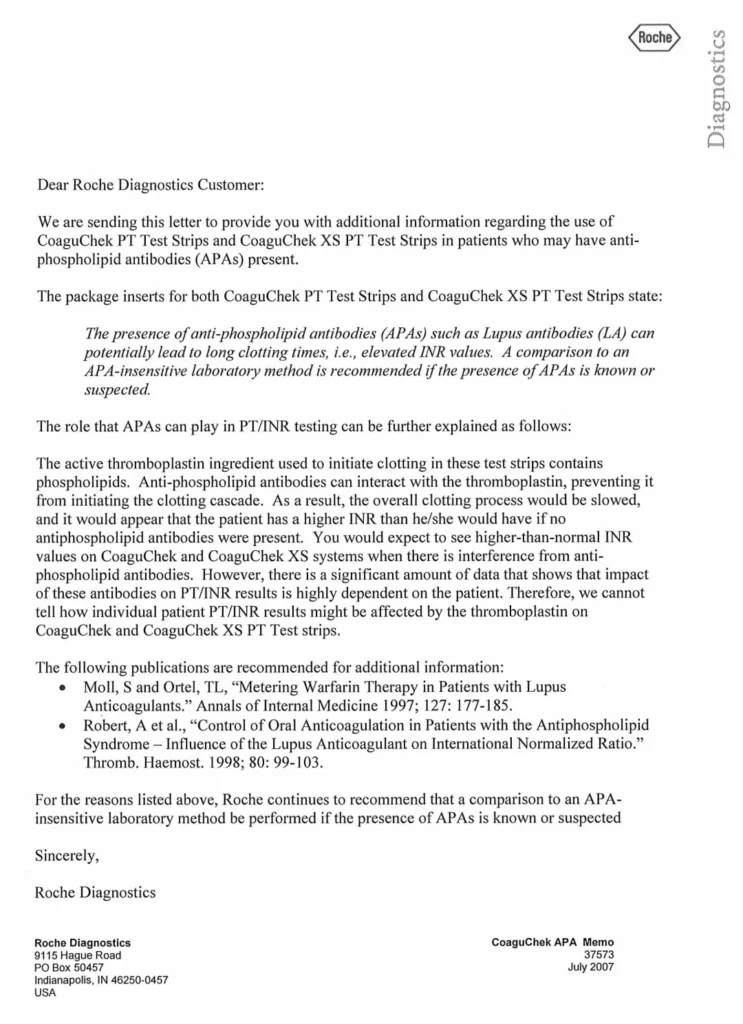
The presence of antiphospholipid antibodies (APAs) such as Lupus antibodies (LA) can potentially lead to long clotting times, i.e., elevated INR values. A comparison to an APA-insensitive laboratory method is recommended if the presence of APAs is known or suspected
The role that APAs can play in PT/INR testing can be further explained as follows.
The active thromboplastin ingredient used to initiate clotting in these test strips contains phospholipids
Antiphospholipid antibodies can interact with the thromboplastin, preventing it from initiating the clotting cascade. As a result, the overall clotting process would be slowed, and it would appear that the patient has a higher INR than he/she would have if no antiphospholipid antibodies were present. You would expect to see higher-than-normal INR values on CoaguChek PT and CoaguChek XS systems when there is interference from antiphospholipid antibodies. However, there is a significant amount of data that shows that impact of these antibodies on PT/INR results is highly dependent on the patient. Therefore, we cannot tell how individual patient PT/INR results might be affected by the thromboplastin on CoaguChek PT and CoaguChek XS PT Test strips
Source: Roche