Antiphospholipid Syndrome (APS) | APSFA
- Introduction
- What is Antiphospholipid Syndrome?
- APS Is an Autoimmune Disease
- APS: The Statistics
- Clinical Features of APS
- How is APS Diagnosed?
- APS Treatment and Prevention
- Doctors and Information on APS
- Women & APS
- Other Points to Consider
- Safety When Traveling
- Take Your Medication
- Symptoms to Watch For
- Coping with APS
- How Can You Help?
- Disclaimer
Introduction
This page is a layman’s terms summary of Antiphospholipid Syndrome (APS). It covers such topics as diagnosis, symptoms, treatment, and coping. It is meant for patients newly diagnosed; however, it would also be good for informing friends and family about your disease.
What is Antiphospholipid Syndrome?
Antiphospholipid Syndrome or APS is an autoimmune disorder in which the body recognizes certain normal components of blood and/or cell membranes as foreign substances and produces antibodies against them. Patients with these antibodies may experience blood clots, including heart attacks and strokes, and miscarriages. APS may occur in people with systemic lupus erythematosus, other autoimmune diseases, or in otherwise healthy individuals.
APS is formerly known as APLS, APLA, Hughes Syndrome, or “Sticky Blood.”
APS is an Autoimmune Disease
One way our immune system fights infections is by producing antibodies. Antibodies are proteins in the blood and body fluids that bind to foreign invaders, such as bacteria and viruses, and help the immune system destroy and remove them. Sometimes the immune system doesn’t function properly and makes antibodies against normal organs and tissues in the body. These self-reactive antibodies are called autoantibodies. The autoantibodies in APS were originally thought to recognize that recognize certain phospholipids, fatty molecules that make up part of normal cell membranes, hence the name “antiphospholipid” antibodies. It is now known that most autoantibodies in APS patients recognize blood proteins that bind to phospholipids, rather than phospholipids themselves. Two blood proteins that are major targets of antiphospholipid antibodies are 2-glycoprotein I and prothrombin.
APS: The Statistics
- Number 1 cause of stroke in young people.
- 20% of all cases of blood clots in large veins (deep vein thrombosis), including blood clots that go to the lungs (pulmonary embolism), are due to APS.
- 1 out of 5 women with recurrent miscarriages has APS.
- One third of strokes occurring in younger people (under the age of 50) are due to APS.
- APS is a major women’s health issue: 75-90% of those affected by APS are women.
- 40-50% of patients with APS also have Lupus.
- Antiphospholipid Syndrome affects nine women for every man.
- It is estimated that, as of 2019, it affects 1 in 2000 Americans.
Clinical Features of APS
People with antiphospholipid antibodies have an increased risk of developing one or more of the following problems:
- Blood clots in veins, particularly deep vein thrombosis (DVT)
- Blood clots that go to the lungs (pulmonary embolism)
- Blood clots in the arteries
- Miscarriages—these can occur at any stage of pregnancy, but are most common in the late first trimester or early second trimester
- Pre-eclampsia, eclampsia, fetal growth retardation, premature delivery
- Heart attacks, angina
- Strokes
- Brief stroke-like episodes called transient ischemic attacks (TIAs), for example, loss of vision
- Decreased levels of platelets (small blood cells involved in blood clotting)
- Heart valve problems, sometimes requiring valve surgery or valve replacement
- Persistent or transient blotchy, lacy bluish rash (livedo reticularis)
- Skin ulcers, most commonly on the legs or feet
- “Catastrophic” APS—a very rare, life-threatening syndrome in which clots form in small blood vessels of multiple organs (such as heart, lungs, brain, kidneys)
Other features that might be associated with antiphospholipid antibodies include:
- Problems with thinking clearly (loss of concentration, difficulty with reading comprehension and performing calculations, and memory loss)
- Neurological problems similar to multiple sclerosis.
- Migraine headaches, sometimes with visual disturbances
- Other neurological symptoms include episodes of partial or total vision loss, dizziness, vertigo, loss of balance, seizures, and other abnormal movements
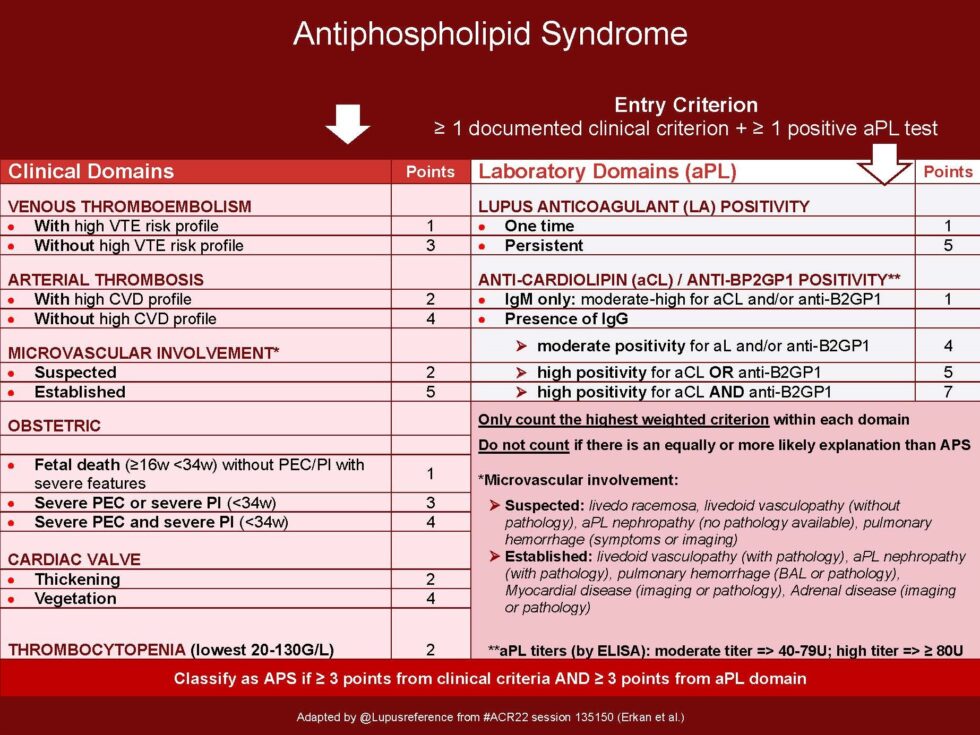
How is APS Diagnosed?
Physicians use a combination of clinical symptoms (see above) and laboratory tests to diagnose APS. The common blood tests for antiphospholipid antibodies are as follows:
- Anticardiolipin antibodies (IgG and IgM)
- Lupus anticoagulant—a panel of blood clotting tests that may include the dilute Russel Viper venom time (dRVVT), lupus aPTT, mixing studies, and hex phase phospholipid test, platelet neutralization procedure
- Antibodies to b2-glycoprotein I (IgG, IgM, IgA)
Panels of tests for antibodies to phospholipids other than cardiolipin are available but have not undergone the rigorous international standardization efforts applied to anticardiolipin assays. A number of experts in the field question the usefulness of these panels, which may be quite expensive.
If you test positive for any of the above tests, testing will be done 12 weeks later to confirm your diagnosis.
APS Treatment and Prevention
There is no cure for APS, but there is treatment. The treatment of choice for patients with APS who have had a blood clot is anticoagulant therapy. This is usually successful in preventing further clots. For women with APS and recurrent miscarriages who have not had a prior blood clot, the use of anticoagulant therapy during pregnancy significantly increases the likelihood of a successful outcome. Some individuals may have elevated levels of antiphospholipid antibodies but no clinical manifestations of the syndrome. These individuals are usually treated with aspirin. Aspirin reduces the risk of blood clots by making the platelets less sticky. Studies are ongoing to determine the effectiveness of aspirin and whether low-dose anticoagulants might be more effective.
In general, patients who have had a blood clot (i.e., stroke, heart attack, DVT) and have persistently positive tests for antiphospholipid antibodies should be treated with anticoagulants indefinitely. Discontinuing treatment after a fixed period, such as 6 months, may be quite dangerous in these patients. In some patients with a history of blood clots, antiphospholipid antibodies may disappear over time. It is not known whether it is safe to stop anticoagulation in this situation. Consultation with a doctor experienced in treating APS is recommended for such patients.
The treatment of at-risk patients may not always include anticoagulants but may include dietary changes, behavior modification, and/or treatment of associated conditions. Do not smoke or do drugs; drink plenty of water, watch your weight, and exercise, if possible.
Doctors and Information on APS
Although APS is actually one of the more common autoimmune diseases, some primary care doctors remain uninformed about it. When their patients have symptoms of APS, these doctors may not test for antiphospholipid antibodies soon enough or at all. Unfortunately, many patients have had to see several physicians and specialists before receiving an accurate diagnosis and treatment.
The type of doctor a patient sees should be determined by the patient’s symptoms, and any given patient may benefit from the input of several specialists. For patients with blood clots, a hematologist would often be involved in managing anticoagulant therapy (blood thinner). For patients with recurrent miscarriages, a high-risk obstetrician should be consulted. For patients who also have rheumatologic symptoms, such as symptoms of lupus, a rheumatologist would be important to see. Of course, all patients would benefit from having a single physician as their primary care provider to coordinate their health care needs.
Women & APS
APS and Pregnancy Complications
Women with APS may have difficulties with pregnancy. During pregnancy, women are at higher risk of developing blood clots and preeclampsia. In APS, pregnancies are thought to be lost because blood clots form in the placenta and starve the baby of nutrition. Some women may have trouble getting pregnant, while others may experience repeated miscarriages. Blood clots that develop in the placenta can cause fetal growth problems, fetal distress, preterm birth, or pregnancy loss.
Expert care and close monitoring of the pregnancy are essential with a doctor knowledgeable about APS. During pregnancy, physicians may recommend low-dose aspirin and daily injections of the blood-thinning drug heparin. This gives the fetus about an 80% chance of survival, a drastic improvement from the 1980’s when fetal survival was around 20%. The therapy is started at the beginning of pregnancy and halted just before delivery to reduce the risk of bleeding during childbirth. Soon after birth, treatment resumes for about six weeks due to an increased risk of clotting in the postpartum period. In a more serious case, preeclampsia may set in towards the end of pregnancy, and a planned premature birth may be necessary. Heparin can cause bone loss, so women may need to take additional calcium during pregnancy. In addition, women need to be monitored for the development of a low platelet count.
Over the long term, many doctors recommend women continue to take a low dose of aspirin to reduce the risk of developing dangerous blood clots. Many women with APS are unaware they have the condition, but it can be diagnosed with a blood test. Doctors may consider the diagnosis when a woman has repeated, unexplained pregnancy loss.
If you are trying to get pregnant or are pregnant, it is very important to let your doctor know immediately. Continued use of warfarin may cause birth defects. The doctor will change your medication to a different, safe blood thinner. Using proper treatment, women with APS have about the same risks as other women during pregnancy.
APS pregnancies are not normal. A normal pregnancy is 40 weeks. In APS, it is more common to deliver the baby between 30-35 weeks, and between 3-5 pounds. Heparin partially protects the placenta, but not fully, so the baby receives enough nutrition to survive longer in the mother. Once born, the babies do fine.
Many women who have problems with APS during pregnancy are completely fine when not pregnant. Others do go on to develop clotting problems. Currently, there is no way of telling which women will be unlucky until a clot actually occurs.
Infertility has also been linked to antiphospholipid antibodies. Testing for these antibodies is becoming routine in infertility clinics.
Birth Control Pills & Hormone Replacement Therapy
Women also need to avoid estrogen therapy (such as birth control or hormone replacement therapy) because estrogen predisposes patients to clotting.
Other forms of contraception should be discussed with your doctor.
Problems with Periods
Some women taking warfarin experience problems with increased bleeding. It can lead to anemia. Tell your doctor about this problem. The doctor can recommend several options to prevent anemia. One example is: for women who have already given birth and are not actively trying to conceive, the Mirena® IUD has been successful in reducing menstrual blood loss. As it only releases hormones to the uterus lining and is not absorbed into the bloodstream, it is safe for women with APS to use.
Other Points to Consider
You may notice you bruise more easily, or little cuts will bleed longer when you are taking anticoagulants. Injuries can be more serious when on anticoagulants, and care should be taken during any activity that can result in injury. Contact sports are not recommended.
If, while on anticoagulants, you injure your head, go directly to the Emergency Room. Your brain is very sensitive to bleeding while on anticoagulants. If a serious injury occurs, go directly to the Emergency Room and make sure they know you are taking anticoagulants, and tell them your most recent INR if you are on warfarin.
You should wear a Medical Alert bracelet at all times. You can order one through Medic Alert. A bracelet is the most visible, easiest, and most recognized; however, necklaces and other options are also available.
Safety When Traveling
Long trips, especially by air, have some clotting risk even for non-APS people. It is important for people with APS to get up and walk around at least every couple of hours. On a long car trip, stop at least every two hours and walk. Drink plenty of water and wear compression stockings to help reduce your chance of DVT. If you plan to be away during a periodic blood test, arrange for the test before you leave for the trip.
Take Your Medication
It is very important to take your medicine every day. Try to take your medicine at the same time each day for consistency. You may want to get a pillbox that holds at least one week’s supply of the pill(s) or mark it on a calendar when you take your medicine. This will help you to know when you have taken your pills. Do not take two doses in one day if you have forgotten your dose.
Symptoms to Watch For
If you test positive for APS antibodies, you should be aware of the symptoms caused by blood clots. If any of these symptoms occur, seek medical help immediately. Symptoms that could be caused by a blood clot include:
Heart Attack
Heart attack symptoms include chest discomfort or pain. Most heart attacks involve discomfort in the center of the chest that lasts more than a few minutes, or that goes away and comes back. It can feel like uncomfortable pressure, squeezing, a sense of fullness, or pain. Generally, it becomes so bad that it may feel unbearable and relentless, but occasionally the pain can be milder.
- Discomfort in other areas of the upper body. Symptoms can include pain or discomfort in one or both arms, the back, neck, jaw, or stomach.
- Shortness of breath. This feeling often comes along with chest discomfort. But it can occur before the chest discomfort.
- Other signs may include breaking out in a cold sweat, nausea, or light-headedness.
- But also be aware that there are different symptoms for women, such as anxiety, nausea & vomiting, heart palpitations, unusual & unexplained fatigue, dizziness & fainting, jaw, neck or upper back pain, and not always chest pain.
Stroke
Strokes (Blood clots in the brain) can be life-threatening. Some stroke symptoms may last only minutes or a few hours and are called TIA’s. (Transient Ischemic Attack or mini stroke.) Rapid treatment (within three hours) is vital. Medical treatments that reverse the stroke damage are available—but only if you seek immediate treatment. Stroke symptoms are:
- Sudden numbness or weakness of the face, arm, or leg, especially on one side of the body.
- Sudden confusion, trouble speaking, or understanding speech.
- Sudden trouble seeing in one or both eyes.
- Sudden trouble walking, dizziness, loss of balance, or coordination.
- Suddenly, a very severe headache with no known cause. It can also be a very severe headache that lasts for days.
Clots in other locations
Muscle pain, numbness, or tingling, pale color, weakness, or muscle spasm in a leg or arm.
- The arm or leg feels cold, hot, or swollen to the touch. May feel like a muscle strain.
- Extreme pain without a cause, anywhere in the body.
- Shortness of breath, or chest pain (under the breast bone or on one side of the chest) may radiate outward from the chest. (This could indicate a clot in the lungs or a heart attack.)
- Sudden heavy cough, especially if you cough up blood.
- Rapid breathing.
Heart attacks, strokes, and other blood clots need immediate medical attention. Go immediately to the Emergency Room.
If you feel these warning signs, DIAL 911 IMMEDIATELY. Most people wait 2 or 3 hours before seeking care, yet by then the heart may suffer significant damage. Dial 911 within 5 minutes if you or someone with you experiences these symptoms.
Coping with APS
APS treatment is lifelong. The benefits of treating blood clots caused by APS outweigh the treatment’s minor side effects.
Most of the time, people with APS will appear on the outside just as they did before they were diagnosed. Because of this, it may be difficult for family and friends to understand that you have a life-threatening illness and that you just can’t do some of the things that you could before. They can’t see what is going on with your body, which can be quite frustrating on both ends.
In some cases, you may want a therapist to help you adjust. Any person with a life-threatening disease is at risk of being depressed. In some cases, this progresses to clinical depression. It is very important to discuss your mental health with your doctor as well as your physical health.
The APS Foundation of America, Inc has a place on the Internet where you can communicate with others who have this disease. Find our support forum here. You are the only one who knows exactly how you feel. Others with the same disease are very understanding, and support groups of some kind can make your life much fuller. Your immediate family and children should be told about your disease, how it affects you, what it means to them, as well as what you may have to expect of them in support.
The good news is that many people with proper treatment live normal, full lives. Others may find their lives changed forever due to APS, but a positive attitude will mean that life can still be worthwhile and fulfilling as the correct treatment prevents further problems.
How Can You Help?
There are many ways you can help the APS Foundation of America, Inc. You can volunteer your time & talents, such as in the area of fundraising, advocacy, finance, or support group experiences, donate money, or purchase APS gear through our webpage, our CafePress store, or our WooCommerce Shop. where 100% of the profits from its products go to the APSFA. We also have an Amazon Store for APS- and chronic illness-related items, where a small percentage of the profits from these products go to the APSFA.
The APS Foundation of America, Inc is a non-profit organization.
Without your generous donations, the APSFA could not continue to provide APS patients and their families with the information on our foundation page and social media pages, support Antiphospholipid Syndrome (APS) research – both adult and pediatric, obtain education on APS and related diseases through various mediums, and share that with the APS community and the general community as a whole. In addition, we are continuing to develop a strategic plan for the future of the APSFA and plan to raise funds toward our long-term goals.
Thank you in advance for your support and time. Please contact us through our website or call 608-782-2626 for more information.
Please send donations to:
APS Foundation of America, Inc
c/o Tina Pohlman
624 10th St N #4
La Crosse, Wisconsin 54601
We also accept PayPal donations via our website.
We thank you for your support!
Disclaimer
APS Foundation of America, Inc. is not intended to replace standard doctor-patient visits, physical examination, and medical testing. Information given to members is only an opinion. All information should be confirmed with your personal doctor. Always seek the advice of a trained physician in person before seeking any new treatment regarding your medical diagnosis or condition. Any information received from APS Foundation of America, Inc is not intended to diagnose, treat, or cure. This brochure is for informational purposes only.
If you think you may have a medical emergency, call your doctor or 911 immediately.
A team of people contributed to this publication. Information was adapted from various websites, books, and other media sources. This pamphlet was assessed at the draft stage by doctors, allied health professionals, an education specialist, and people with APS. A non-medical editor rewrote the text to make it easy to understand, and an APS Foundation of America, Inc. medical editor is responsible for the content overall. Copyright 2006 Bibliography